Description
Introduction
Long-term impact of total knee arthroplasty (TKA) on mortality rates has been inconsistent according to various reports. While some studies have indicated that TKA can lower long-term mortality rates in elderly patients, they have also highlighted contrasting higher mortality outcomes associated with TKA in patients younger than 60. Such findings were explained by possible over-representation of patients who were less healthy for joint replacement. The aim of this study is to examine mortality rates in TKA patients under the age of 60 with a minimum 12-year follow-up and compare them to those in the general population. Additionally, we reviewed cause of death and analyzed the predictors of death among the deceased patients. Long-term implant survival outcomes were also investigated.
Methods
We retrospectively investigated patients under the age of 60 with primary knee osteoarthritis (OA) who received TKA (n=152) in a single institution from July 2005 to December 2011, with a mean follow-up period of 14.5 years. Patient demographics, preoperative comorbidity, and clinical parameters were reviewed based on medical records. Korea National Statistical Office provided information on survival status as of May of 2023 and the cause and date of death of the deceased patients. Mortality was assessed using the person-year approach. The expected number of deaths within specific age and sex groups was calculated from mortality data from the Korean general population. Standardized mortality ratios (SMR) were then computed with corresponding 95% confidence intervals (CI) assuming that the observed deaths followed a Poisson distribution. Kaplan-Meier estimates and a Cox proportional hazard model were employed for the analysis of survivorship and predictors for mortality.
Results
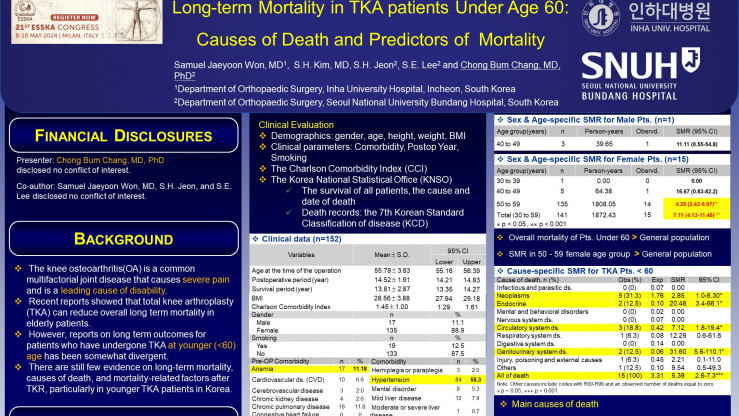
A total of 16 patients (10.5%) deceased during the follow-up period. The overall mortality in the cohort was higher than that in the general population (SMR: 3.3; 95% CI: 2.0-5.3; p<0.001). Specifically, female patients between age 50 and 59 showed significantly higher mortality rate than the general population. (SMR: 7.1; 95% CI: 4.1-11.5; p<0.001) The deceased patients had a higher smoking prevalence as well as higher preoperative Charlson comorbidity index (CCI) score than the surviving patients, but no differences was found in BMI, sex, and age. Cox hazard regression analysis suggested that preoperative comorbidities including smoking (HR=7.47; p=0.001), myocardial infarction (HR=12.1; p=0.01), anemia (HR=10.0; p=<0.001), metastatic cancer (HR=15.34; p=0.022) are predictors for mortality in younger TKA patients. A total of 6 patients (3.9%) underwent revision surgery, and the reason for revision was infection (n=3, 50%) and fracture (n=3, 50%). None of the patients required revision surgery for aseptic loosening or polyethylene wear.
Conclusion
In our study cohort, none of the TKA patients under the age of 60 required revision surgery for aseptic loosening or polyethylene wear. However, they had a higher mortality rate compared to the age-matched general population. These findings suggest that continuous surveillance and management of overall health is necessary for a younger patient with severe primary knee OA.